


مشاوره محصول
آدرس ایمیل شما منتشر نخواهد شد. فیلدهای الزامی علامتگذاری شدهاند *
 انگلیسی
انگلیسی


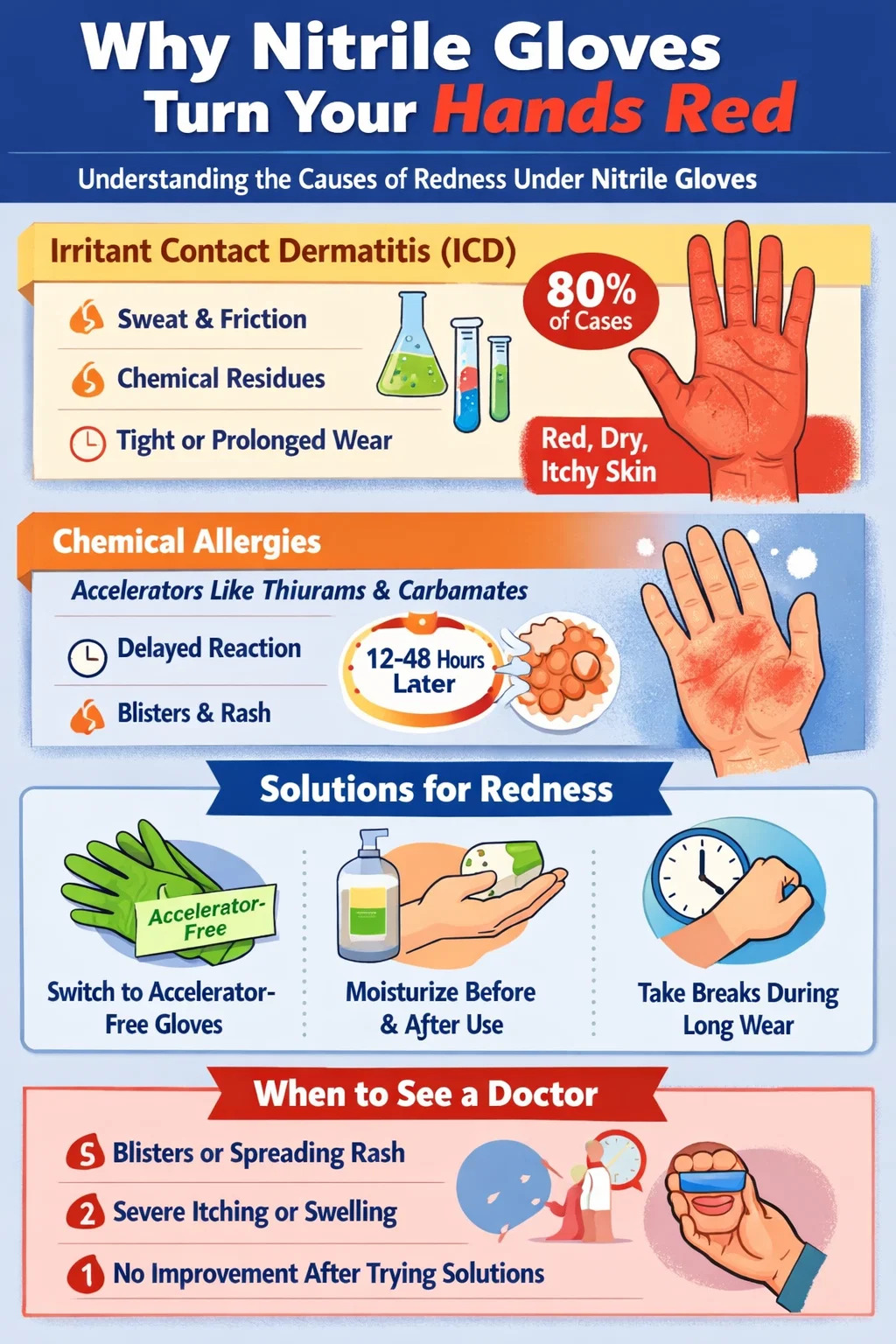
If your hands turn red after wearing nitrile gloves, the most likely cause is irritant contact dermatitis — a non-allergic skin reaction triggered by friction, heat, sweat buildup, or residual chemicals on the glove surface. This accounts for roughly 80% of all glove-related skin complaints. A smaller portion of people experience a true allergic response, either to chemical accelerators used during the manufacturing process or, in rare cases, to the nitrile polymer itself. The redness can also result from something as simple as gloves that are too tight, worn too long, or not removed correctly.
Nitrile is widely marketed as the latex-free alternative, and it genuinely is safer for people with latex allergies. But "latex-free" does not mean "reaction-free." Understanding exactly which mechanism is causing your red hands is the first step toward fixing the problem — and in most cases, it is fixable without giving up glove protection entirely.
Irritant contact dermatitis (ICD) is not an allergy. It is a physical breakdown of the skin's protective barrier caused by repeated mechanical or chemical stress. When you wear nitrile gloves, several things happen simultaneously that set the stage for ICD:
Studies published in occupational health journals consistently find that healthcare workers — one of the highest-frequency glove-wearing populations — report skin complaints at rates between 25% and 55%, with ICD responsible for the majority. The condition presents as redness, dryness, scaling, and a burning or tight sensation. It tends to be confined to the area directly covered by the glove, most often the back of the hand and fingers.
ICD is cumulative. Wearing gloves for 30 minutes once a week produces almost no reaction in most people. But wearing them for 6–8 hours per day, five days a week, creates enough repeated disruption that even healthy skin starts to show signs of irritation within a few weeks.
Nitrile rubber does not vulcanize on its own. To convert the raw nitrile polymer into the stretchy, durable glove you wear, manufacturers add chemical accelerators during production. The most commonly used classes are:
These chemicals can leach out of the finished glove and come into prolonged contact with the skin. In individuals who have developed a sensitivity — through repeated low-dose exposure over time — the immune system mounts a Type IV delayed hypersensitivity response. This is a form of allergic contact dermatitis (ACD).
The critical distinction between ICD and ACD lies in timing and distribution. ICD typically begins within minutes to an hour of glove contact, stays localized to the contact zone, and resolves quickly after gloves are removed. ACD, by contrast, often appears 12 to 72 hours after exposure, can spread beyond the glove contact area, and frequently produces small fluid-filled blisters (vesicles) alongside the redness. Patch testing by a dermatologist is the only reliable way to confirm which accelerator chemicals you are sensitive to.
Research from contact dermatitis clinics in Europe and North America has found thiuram sensitivity rates of 5–10% in the general population and significantly higher among healthcare workers who wear gloves daily. Carbamate sensitivity is less common but increasingly recognized as manufacturers substitute carbamates for thiurams in response to consumer demand.
In response to growing evidence of accelerator-related ACD, several manufacturers now produce accelerator-free nitrile gloves that use alternative vulcanization chemistry — typically electron-beam or UV-curing processes. Brands like Ansell GAMMEX, Sempermed, and Kimberly-Clark offer accelerator-free lines primarily aimed at medical and surgical markets.
Clinical studies evaluating these products in sensitized individuals have shown meaningful improvement: in one prospective trial, over 70% of participants with confirmed thiuram allergy reported complete resolution of their glove-related dermatitis after switching to accelerator-free nitrile gloves. These gloves cost more — often 30–60% above standard nitrile — but for people with genuine ACD, the investment eliminates the root cause rather than just managing symptoms.
Even when chemistry is not the issue, the way gloves are worn has a substantial impact on whether your hands redden. These physical factors are often overlooked but easy to address:
Wearing nitrile gloves that are too small compresses the hand, restricts circulation, and increases friction at the fingertips and knuckle creases. Too large, and the glove bunches and twists with movement, creating repeated abrasion points. Most manufacturers produce sizes XS through XL or XXL. Measure your dominant hand across the widest part of the palm (excluding thumb) in inches: under 7 inches is typically a small, 7–8 inches a medium, 8–9 inches a large, and over 9 inches an XL.
The skin's moisture content inside a glove rises sharply after about 20 minutes of wear. Extended sessions lasting 2+ hours create a warm, humid microenvironment that degrades the skin barrier. When work requirements demand extended glove use, taking short breaks of 5–10 minutes every hour to remove gloves and allow skin to dry significantly reduces ICD severity.
Putting on nitrile gloves over hands that still have soap, sanitizer, or water on them traps those substances against the skin for the duration of wear. Alcohol from hand sanitizers is particularly irritating under occlusion. Always allow hands to dry completely before gloving — ideally for at least 30 seconds after drying with a towel.
Yanking gloves off by the fingertips snaps the material against the skin repeatedly. The correct method — gripping the outside of one glove near the wrist, peeling it off inside-out, then using the bare fingers of that hand to slide under the cuff of the remaining glove — minimizes mechanical trauma to skin. In high-frequency removal situations (changing gloves between every patient, for example), this adds up meaningfully over a shift.
It helps to understand where nitrile sits on the spectrum of glove-related skin reactions compared to other common materials:
| Glove Material | ICD Risk | Allergic Risk (Type IV) | Allergic Risk (Type I) | Primary Allergens |
|---|---|---|---|---|
| Natural Rubber Latex | Moderate | High | High | Latex proteins, thiurams, carbamates |
| Nitrile (standard) | Moderate | Moderate | Very Low | Thiurams, carbamates, MBT |
| Nitrile (accelerator-free) | Low–Moderate | Very Low | Very Low | Minimal residual chemicals |
| Vinyl (PVC) | Low | Low | Very Low | Plasticizers (rare) |
| Neoprene | Low–Moderate | Low | Very Low | Thiurams (less common) |
Nitrile's advantage over latex is real and significant when it comes to Type I (immediate) allergic reactions — the kind that can cause hives, swelling, and in severe cases anaphylaxis. But for contact dermatitis, nitrile is not dramatically better than latex. The accelerator chemicals used in both materials overlap substantially, meaning someone who develops a thiuram allergy from latex gloves may find the same chemical waiting for them in a standard nitrile glove.
Whether the cause is ICD or a mild accelerator sensitivity, the condition of your skin before, during, and after glove wear affects how severe and persistent the redness becomes. A consistent skin care routine is not optional for frequent glove users — it is occupational maintenance.
Apply a non-greasy barrier cream or lotion containing ingredients like dimethicone, glycerin, or ceramides. These form a partial protective layer between the skin and the glove environment. Avoid petroleum-heavy products immediately before gloving — petroleum-based emollients can degrade nitrile material over time and may also make the glove interior slippery and harder to control.
A 2019 study in the British Journal of Dermatology found that healthcare workers who applied a glycerin-containing barrier cream before gloving had a 35% lower incidence of ICD compared to a control group that did not use any pre-glove preparation over a 12-week period.
Immediately after removing gloves, rinse hands with lukewarm (not hot) water and pat dry — do not rub, as rubbing on already-compromised skin adds mechanical irritation. Apply a fragrance-free emollient moisturizer within two minutes of drying. The skin's ability to absorb moisturizing ingredients peaks in the brief window after washing when pores are open and the barrier is temporarily softened.
Ingredients to look for in a post-glove moisturizer include ceramide NP, hyaluronic acid, urea (at concentrations of 5–10%), and shea butter. Avoid fragrances, dyes, and preservatives like methylisothiazolinone — all known skin sensitizers that can worsen existing irritation.
If redness persists after a day of glove use, wearing thin cotton glove liners overnight after applying a thick emollient ointment (like petroleum jelly or a ceramide-heavy cream) creates an occlusive environment that accelerates barrier repair. The skin regenerates its lipid barrier most actively during sleep. Repeated overnight treatments for 3–5 nights can noticeably reduce baseline skin irritation, making daytime glove use less provocative.
Most mild redness from nitrile gloves resolves on its own with a few days of rest and proper moisturizing. But certain presentations warrant professional evaluation, and ignoring them can allow a manageable condition to become a chronic occupational health problem.
A dermatologist will typically perform a patch test series using the European Baseline Series or a rubber chemical series to map exactly which chemical compounds are responsible. This information is directly actionable — it tells you which glove types to avoid and which are safe, with precision that no amount of trial-and-error glove switching can replicate.
Pulling everything together into a practical sequence, here is what to do based on how your reaction currently presents:
For people in occupations that mandate glove use — surgeons, food handlers, lab technicians, cleaning staff — complete glove avoidance is not a realistic option. In these cases, the most effective approach combines accelerator-free nitrile gloves with thin cotton inner liner gloves to create a buffer between skin and glove material, a rigorous twice-daily moisturizing protocol, and prescription-strength barrier or corticosteroid treatment on days when the skin is particularly reactive. A dermatologist familiar with occupational skin conditions can build a maintenance regimen that keeps the skin functional while protecting both the worker and the people they serve.
One question that comes up frequently is whether the blue, black, purple, or teal coloring of nitrile gloves contributes to skin redness. The colorants themselves — typically azo dyes or carbon black for darker gloves — are not known primary causes of contact dermatitis in most people, though rare dye-specific sensitivities have been documented in dermatology literature. The color of the glove is generally not a reliable predictor of how skin-friendly it will be.
Brand and manufacturing quality matter more. Budget-tier nitrile gloves produced without rigorous post-leaching processes (a step where finished gloves are soaked to wash out residual chemicals) tend to have higher extractable chemical content. Premium medical-grade gloves are subject to stricter regulatory standards — EN 455 in Europe and ASTM D6319 in North America specify limits on residual proteins and certain chemicals. Choosing gloves that meet or exceed these standards reduces but does not eliminate chemical exposure.
Some manufacturers now publish accelerator chemical test results for their products. If skin sensitivity is a recurring issue, requesting this data — or choosing brands that advertise "low-chemical" or "accelerator-free" formulations — is a concrete step that cuts through marketing language and addresses the actual chemistry responsible for most non-trivial glove reactions.
چه چیزی جایگزین دستکش های لاتکس شد؟ جایگزین های برتر توضیح داده شده است
دستکش نیتریل در مقابل لاتکس: کدام یک برای شما ایمن تر است؟
آدرس ایمیل شما منتشر نخواهد شد. فیلدهای الزامی علامتگذاری شدهاند *
شماره هنر: FY.2521
میتوانید از طریق این فرم با من تماس بگیرید.

















